The last nail in the coffin of Covid boosters
“The true effectiveness of the first booster was short-lived, if meaningful at all. Peak protection was somewhere between mediocre and zero, and it is impossible to narrow that range.”
That was my conclusion after analyzing the effectiveness of the first booster (reposted on Brownstone and The Daily Sceptic).
We can try to narrow the range by analyzing the merit of another booster, the fourth dose, as compared with three previous doses. I will show here that its effectiveness was close to zero, with an upper bound around 15%. Whether it was exactly zero, 5%, or 15%, makes no difference. That’s not a basis for mass vaccination.
My analysis of the first booster was based on removing one of two key biases, which is called the healthy vaccinee bias. That strong bias results from the fact that people who take a vaccine (whether against flu or against Covid) are healthier, on average, than people who do not, even in narrow age bands, and even among residents of nursing homes. Therefore part, or all, of their lower Covid mortality is not the vaccine effect. They are simply healthier people than their unvaccinated counterparts.
To remove the healthy vaccinee bias, we adjust the risk of Covid death in vaccinated upward, using data on non-Covid death, and thereby create two groups that are comparable on their baseline risk of death. (Mathematically, it is equivalent to downward adjustment of the Covid death risk in unvaccinated.)
The method is not perfect, but it does get us much closer to the truth than naïve comparisons of vaccinated with unvaccinated, which have been presented on countless dashboards. Moreover, in the absence of randomized trials of the mortality endpoint, that method is likely superior to observational studies that try to adjust for, or match on, a limited number of health-related variables. Such adjustments proved unsatisfactory in the case of flu vaccines and recently in the case of the first booster.
My largest source for the first booster (third dose) analysis was the dataset of the Office of National Statistics (ONS), England. I used it again to study the effectiveness of the second booster (fourth dose).
Contrary to what some might think, the healthy vaccinee bias is not restricted to a comparison of vaccinated (two doses) with unvaccinated. Three-dose recipients were healthier than two-dose recipients (consistently), and that was the case again with recipients of the fourth dose. They were healthier than three-dose recipients. With one exception, their non-Covid mortality was substantially lower in every age group and every month I analyzed.
The example below shows the healthy vaccinee bias in the ONS data — in one age group (70–79) and one month (December 2022). As you can see, the rate of non-Covid death in four-dose recipients (2476.0) was less than half that rate in three-dose recipients (6579.4). Of course, the second booster was not expected to protect from other causes of death… That’s the evidence of the healthy vaccinee bias.
In the tables below the data, I show two corrected estimates of effectiveness. The count-based estimate (left table) is not prone to miscalculation of person-years, which occasionally happened in the ONS data. It will be used throughout. (I will skip a technical explanation of the computation.)

The biased estimate of effectiveness is 70% (1— 88.7/298.7). After correction we get mediocre effectiveness of the fourth dose (about 20%), which may still be an overestimation due to another key bias called differential misclassification of the cause of death.
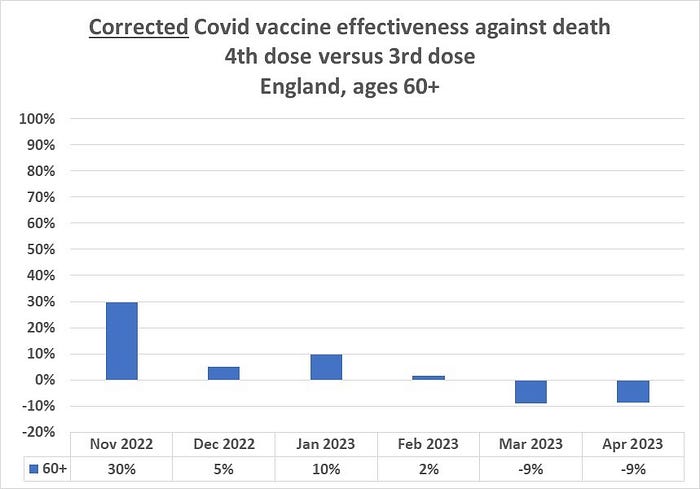
My recent analysis of the first booster effectiveness in the ONS data was confined to age 60 and above, over a six-month period: November 2021 through April 2022. I will examine the second booster effectiveness in the same months, a year later: November 2022 through April 2023. That period contained two small (endemic) Covid waves in England (top figure). The booster uptake is also shown (bottom figure.)


The spread of the corrected, monthly estimates (graph below) is compatible with near zero effectiveness of the second booster. Deviations in either direction should not be over-interpreted. That’s the expected (random) spread of results when the true effectiveness is somewhere near null. The aberrant result in November 2022 might reflect some other bias that is related to the rapid rise of vaccine uptake. There is no other plausible explanation.
Monthly estimates in four age groups are shown in the graph below. By and large, we observe the same near-null spread in each age group, and the same divergence in November 2022.
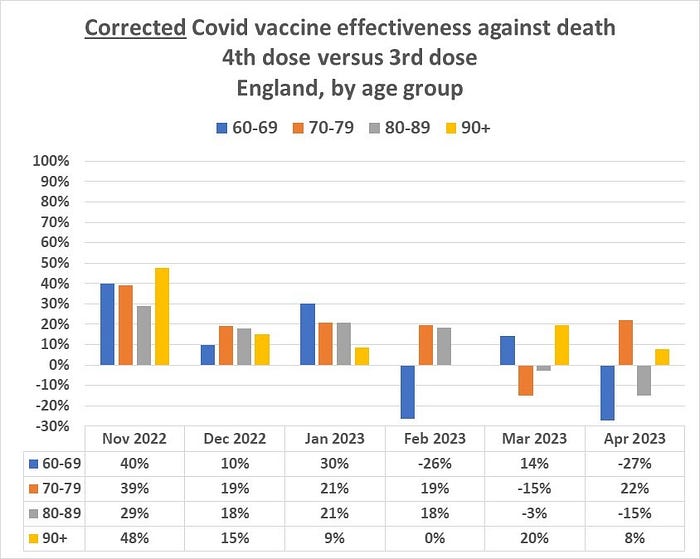
On the assumption of random fluctuation over time — around some nearly stable, small value — we may combine the six-month data for each age group to get a single estimate. (Those with advanced statistical knowledge might be familiar with the bias-variance tradeoff.) As shown below, effectiveness is estimated to be 10-15% or so, assuming complete removal of the healthy vaccinee bias and no other bias. Neither is necessarily true.

As I explained elsewhere, another key bias — differential misclassification of the cause of death — would drive above-zero estimates even closer to zero. Unfortunately, it cannot be easily removed.
In short, a useless, or nearly useless, booster.
In March 2022, Time magazine reported on the upcoming second booster, under the headline “What to Know about a Fourth COVID-19 Vaccine Dose”. A reporter wrote:
“On March 29, the U.S. Food and Drug Administration (FDA) issued an emergency use authorization (EUA) for a fourth dose of Pfizer-BioNTech’s and Moderna’s mRNA vaccines for people 50 and older…”
“The FDA believes this option will help to save lives and prevent severe outcomes among the highest risk patients,” said Dr. Peter Marks, director of the FDA Center for Biologics Evaluation and Research, in a briefing on March 29 [2022].”
The belief was based on “an analysis of emerging data”, which meant pilot work — not a randomized trial with a mortality endpoint. That may be the basis for compassionate use of an experimental drug in a patient, but not for mass vaccination, especially when there are short-term vaccine fatalities and serious adverse effects. To those we should add unknown long-term morbidity and mortality consequences of self-manufactured spike protein and exogenous lipid nanoparticles (the mRNA carriers) in various tissues. No, the vaccine does not remain and degrade at the injection site, as originally promised.
It may very well be that adverse consequences of repeated Covid boosters will vastly exceed temporary small benefits (if any). “Safe and effective”, they are not. They should not be allowed until meaningful effectiveness against death is shown in a randomized trial (with informed consent).
