Epidemiological Evidence of Covid mRNA Vaccine Deaths in the UK Yellow Card Database
Despite thousands of reported deaths after Covid mRNA vaccines in databases such as VAERS in the US and the Yellow Card in the UK, there is no scientific acknowledgment of a cause-and-effect relationship. Official analyses haven’t been rigorous or accurate; they were usually based on imprecise denominators (number of doses) and external comparisons. Indeed, detecting a signal in these databases is a methodological challenge.
I have recently completed writing a book on methodology (which I started twenty years ago…). At least five chapters are related to the analysis I will show below. Nonetheless, I will try to provide intuitive, non-technical explanations and just make reference to relevant chapters.
Theoretical Premises
Consider the two mRNA vaccines, Pfizer and Moderna. If neither increases the risk of short-term death, the risk of death following the Pfizer vaccine shouldn’t be different from the risk of death following the Moderna vaccine. Both should be equal to the background risk without vaccination.
If we estimate associations from a case-control study, the odds ratio of death for the contrast between the two mRNA vaccines should be 1 — for safe vaccines. If it is not close to 1, we have evidence of a causal relationship but we don’t know the true magnitude. We don’t have the unvaccinated to contrast with.
Nonetheless, we can still draw some inference.
On the assumption that one of the two vaccines is safe (odds ratio of 1 versus the unvaccinated), we have estimated the harmful effect of the other. Of course, that’s an unlikely scenario for two vaccines that are based on the same mechanism of action. If so, the effect of one (in contrast with the unvaccinated) is unknown but harmful (odds ratio > 1), whereas the effect of the other is larger than estimated by our odds ratio. At any rate, we infer that both vaccines must have caused deaths.
Study Design
In a typical case-control study of death as the outcome, we select dead cases and alive controls (chapter 25). However, in one of many variations of this complicated design, we may select dead controls (chapter 32). The sample for analysis contains data only on dead people. We may similarly restrict a case-control study to hospitalized patients or to other settings that are linked to the outcome of interest.
Conceptually, a database that is restricted to reported events is similar to a database that is restricted to dead people, to hospitalized patients, and so on. We can estimate odds ratios for various events.
For instance, my re-analysis of reported VAERS data on pregnancy-related adverse events (chapter 39) has found substantially high odds ratios for hemorrhage (4.3–5.3) and miscarriage (2.5–2.7).
Data and Analysis
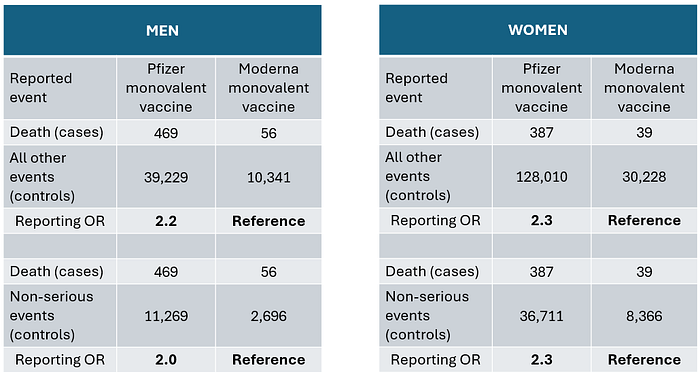
The figure below is an example of relevant raw data from the Yellow Card website. Most of the deaths were reported after the monovalent (original) vaccine. I used the column totals first.

A classical case-control analysis is shown in the table, using two control groups: all non-fatal reported events and only non-serious events. Both approaches lead to a similar result. The odds of reported death after the Pfizer monovalent vaccine are about twice the odds after the Moderna monovalent vaccine. As explained above (theoretical premises), that’s evidence of vaccine-related deaths for one vaccine and most likely for both.

These results are consistent in men and women. (The sum does not match the total above because of missing data in some reports.)
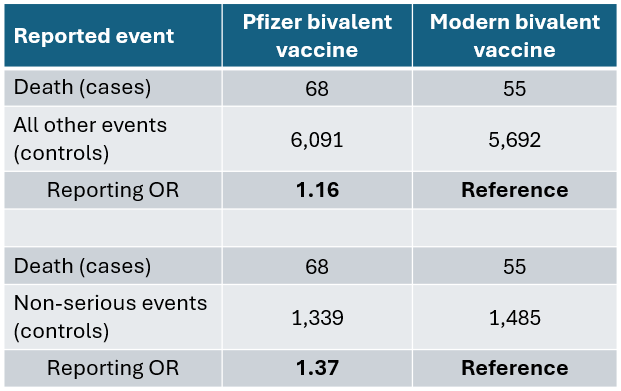
Fewer deaths were linked to the bivalent vaccines. The results are shown below.
A Deeper Insight
The roots of my analysis may be found in a poorly understood measure called the proportional mortality ratio (PMR). Trying to estimate an effect, we divide the proportion of deaths from one cause (out of all deaths) in one group by the corresponding proportion in another. However, the PMR does not correctly estimate an effect, for reasons that are beyond the scope of an intuitive explanation. Still, many epidemiologists continue to teach and compute this measure without alluding to its pitfalls.
The PMR has a close relative called the PRR (proportional reporting ratio), which is used by official agencies and others to detect alarming signals in databases such as VAERS and the Yellow Card. It is just as faulty as the PMR, as pointed out long ago, and may be explained using causal diagrams (chapters 32 and 39).
The correct alternative to both measures is the odds ratio. In our case, it is the reporting odds ratio (ROR), which I computed above. Again, the computation is based on conceptualizing the Yellow Card data as a case-control study.
Of the many threats to validity, two are relevant to the reporting odds ratio: control selection bias and reporting bias. According to a taxonomy of biases, both of them belong to a category called “colliding bias” (chapters 6 and 22). Interestingly, they may operate in opposite directions. Let’s see how.
The controls in my computation were other reported events. It can be shown that if the contrast between the Pfizer vaccine and the Moderna vaccine affects some other events, the odds ratio is biased toward the null (chapter 39). That is, the true odds ratio should be larger than about 2. The ideal control group should include only events that are not affected (or are similarly affected) by the two vaccines, and such events cannot be identified. All that I could have done is to show robust results using two control groups: 1) all reported events other than death; 2) reported non-serious events. In summary, if this bias was operating, I underestimated the magnitude of the true odds ratio.
The second source of potential bias is differential reporting of events. It is best explained by contrasting a covid vaccine with another, non-Covid, vaccine such as a flu vaccine (chapter 39). If an adverse event was reported, it was more likely to have followed a Covid vaccine (new) than a flu vaccine (old, safe). People are more likely to attribute an event to the former. The bias operates to overestimate the adverse effect of a Covid vaccine (larger odds ratio) or to estimate an effect (odds ratio > 1) when it is null. It is, perhaps, the biggest concern when analyzing data from reporting systems.
Fortunately, the second bias is unlikely to operate when we contrast two mRNA vaccines. There is no reason why a death following vaccination was more likely to have been reported if it was a Pfizer mRNA vaccine than a Moderna mRNA vaccine. If so, I computed a conservative estimate due to the first bias. The true odds ratio may be larger than 2.
Consider, for instance, the following hypothetical state of affairs:
- Both vaccines have caused deaths, and the odds ratio for the Moderna vaccine (versus no vaccine) is 2.
- The true odds ratio for the Pfizer vaccine (vs. the Moderna vaccine) is 2.5, not 2.
Then the true odds ratio for the Pfizer vaccine (vs. no vaccine) is 5.
The results for the bivalent vaccines are not striking. Several explanations may be offered. First, the number of deaths is much smaller, so the estimates are more prone to random error. Second, it is possible that the effect is weaker or null for both bivalent vaccines. Lastly, we are estimating the effect in “survivors” of the first vaccination protocol. Perhaps most of those who were susceptible had died after the monovalent dose.
The short-term fatality rate of Covid mRNA vaccines has been real and unacceptable but fortunately not as high as is sometimes assumed. We still don’t know much about long-term effects. There are good reasons to be worried.
Referenced Chapters
Chapter 6: Principles of Causal Diagrams
Chapter 22: Colliding Bias: Misnomers and the Missing Dashed Line
Chapter 25: The Case-Control Study
Chapter 32: Causal Diagrams for the Dead
Chapter 39: The Reporting Odds Ratio and Pregnancy-Related Adverse Events
